Abstract
Objective: To critically reassess the use of botulinum toxin type A (BoNT/A) for gummy smile, with emphasis on anatomical targeting, protocol variability, and the conditions required for reproducible outcome measurement.
Data sources: Literature addressing etiologic phenotyping of gummy smile, elevator-muscle anatomy, BoNT/A formulation and preparation, targeted clinical application, and digital approaches to image-based outcome capture.
Eligibility criteria: Studies and technical sources were prioritized when they directly informed five linked domains: phenotype selection, anatomical rationale, product handling, delivery variables, and the reliability of endpoint documentation.
Methods of synthesis: Critical narrative review integrating anatomical, clinical, pharmaceutical, and measurement-oriented evidence relevant to the translational interpretation of BoNT/A therapy for gummy smile.
Main findings: The literature supports temporary gingival-display reduction in selected muscular cases and offers a credible anatomical rationale for targeting the Yonsei region. However, universality of the point is not supported. Morphometric variation, heterogeneous smile-task architecture, non-equivalent product preparation, and incompletely reported dose-volume-depth relationships remain major interpretive barriers.
Conclusion: BoNT/A remains a defensible minimally invasive option for compatible muscular etiologies, but the field will mature only when anatomical targeting, product handling, dose-volume-depth architecture, smile-task definition, and digitally auditable outcome measurement are integrated within one reproducible protocol.
Keywords: Botulinum toxin type A · gummy smile · Yonsei point · digital workflow · facial imaging · outcome measurement.
Introduction
Among minimally invasive options for gummy smile, botulinum toxin type A (BoNT/A) is attractive because it is reversible, rapid, and often effective in appropriately selected muscular phenotypes. Yet the apparent simplicity of the injection obscures the complexity of the therapeutic system: etiologic selection, landmark choice, formulation, dilution, injected volume, depth, symmetry, and image capture all influence the clinical result.
That complexity is especially consequential in the perioral region. The therapeutic window is narrow, esthetic penalties are immediate, and small technical differences can be mistaken for biologic inconsistency. The result is a literature in which the treatment often seems more reproducible than the endpoint used to judge it.
This review therefore addresses a more stringent question: not simply whether BoNT/A may reduce gingival exposure in selected muscular cases, but which variables determine whether the Yonsei point functions as a reproducible clinical target or remains an anatomical approximation with limited transferability.
Review objective
This review critically reassesses BoNT/A for gummy smile from a translational standpoint. Rather than treating the Yonsei point as an isolated technical maneuver, it examines the interaction among phenotype, anatomy, pharmaceutical handling, and endpoint capture, asking where the current literature is genuinely robust and where it remains methodologically fragile.
Review method and interpretive strategy
This manuscript was prepared as a critical narrative review rather than a systematic review or quantitative synthesis. The literature was selected for direct relevance to five linked domains: etiologic phenotyping of gummy smile, upper-lip elevator anatomy, BoNT/A formulation and preparation, clinical performance of targeted injection strategies, and the reliability of imaging-based outcome capture.
Because the manuscript is intended for a journal situated at the interface of Digital Health and Advanced Biomaterials, evidence was not weighted only by reported clinical effect. Additional interpretive value was assigned to studies that clarified how image acquisition, calibration, metadata structure, or computational post-processing affected endpoint trustworthiness.
Thematic synthesis of the literature
Gummy smile is a clinical presentation, not a unitary diagnosis. Excessive gingival display may reflect vertical maxillary excess, dentoalveolar disproportion, altered passive eruption, lip hypermobility, or hyperactivity of the upper-lip elevator muscles. This distinction is not taxonomic only. It determines whether BoNT/A is mechanistically relevant and therefore whether clinical response can be interpreted as treatment success rather than diagnostic mismatch.
Polo's studies were important not only because they documented reduction in gingival display, but because they made patient selection central to the interpretation of response. Later prospective studies, controlled designs, and pooled analyses support short-term benefit in selected muscular cases, but they do not erase heterogeneity in indication, technique, or outcome capture.
Anatomical basis of the Yonsei point
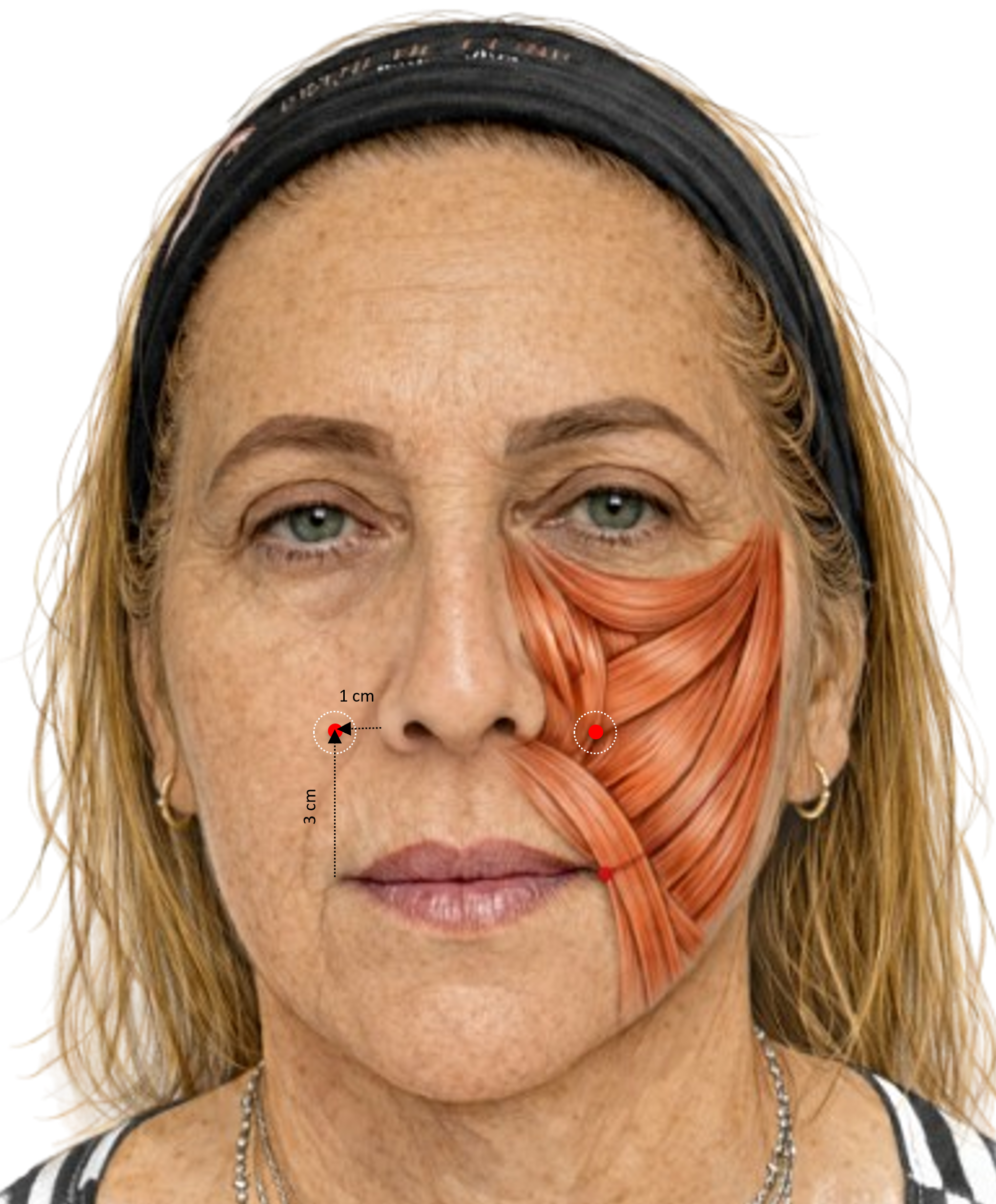
The Yonsei point was a major attempt to subject perioral injection to anatomical reasoning. In the foundational study, Hwang and colleagues mapped the levator labii superioris alaeque nasi, levator labii superioris, and zygomaticus minor, and proposed a single surface target corresponding to their zone of functional convergence. Its procedural simplicity, however, should not be mistaken for universality.
Recent controlled comparison and expert consensus preserve the lateral alar targeting logic, but they also show that injection plane, per-point volume, and measurement workflow must be treated as protocol-defining variables rather than as technical afterthoughts.
Molecular and pharmacological basis of BoNT/A
Any clinical account of BoNT/A must begin with its modular protein architecture. Heavy-chain and light-chain domains mediate neuronal binding, internalization, translocation, and catalytic activity; after entry into cholinergic terminals, the light chain cleaves SNAP-25, blocks acetylcholine release, and produces temporary chemodenervation.
This mechanistic basis matters because the toxin never reaches practice as an abstract molecule. It is used as a formulated, lyophilized, reconstituted, and injected product. Preparation conditions and physicochemical context may therefore contribute to variable clinical expression and should not be treated as negligible background variables.
Clinical evidence and critical interpretation
The clinical literature supports, with moderate consistency, that BoNT/A can temporarily reduce gingival exposure in patients with a predominantly muscular component. What remains unresolved is not whether an effect can occur, but why effect size, symmetry, durability, and esthetic naturalness vary so widely across reports and patients.
The translational problem is therefore not the absence of an anatomical hypothesis, but the persistent mismatch between anatomical plausibility and measurement rigor. Read together, contemporary studies support the Yonsei point as a useful anatomical shorthand, not as a definitive or universally transferable coordinate.
Key studies
| Study | Design | Main contribution | Critical relevance |
|---|---|---|---|
| Hwang et al., 2009 | Anatomical study | Mapped the elevator muscles and proposed the Yonsei point as a zone of functional convergence. | Foundational anatomical rationale without authorizing universalization of the point. |
| Booysen et al., 2023 | Population morphometric study | Demonstrated topographic variability in Yonsei-point standardization. | Strong warning against dogmatic use of the landmark. |
| Gong et al., 2024 | Randomized controlled trial | Compared Yonsei-point injection with classical LLSAN targeting. | Signals more controlled anatomical comparison, but persistent variability remains. |
| Ayaz et al., 2020 | Measurement-reliability study | Compared 2D photography and 3D soft-tissue imaging. | Supports facial metrology as a core translational variable. |
| Rho et al., 2025 | Expert consensus guideline | Recommended small bilateral dosing near the lateral alar region with severity-based adaptation. | Reinforces that point location, plane, and risk architecture must be specified. |
Outcome measurement, digital validity, and translational priority
If one bottleneck runs through this literature, it is outcome measurement. Systematic reviews and meta-analyses repeatedly identify non-equivalent photographic records, heterogeneous follow-up intervals, inconsistent smile tasks, and sparse reporting of calibration or repeatability.
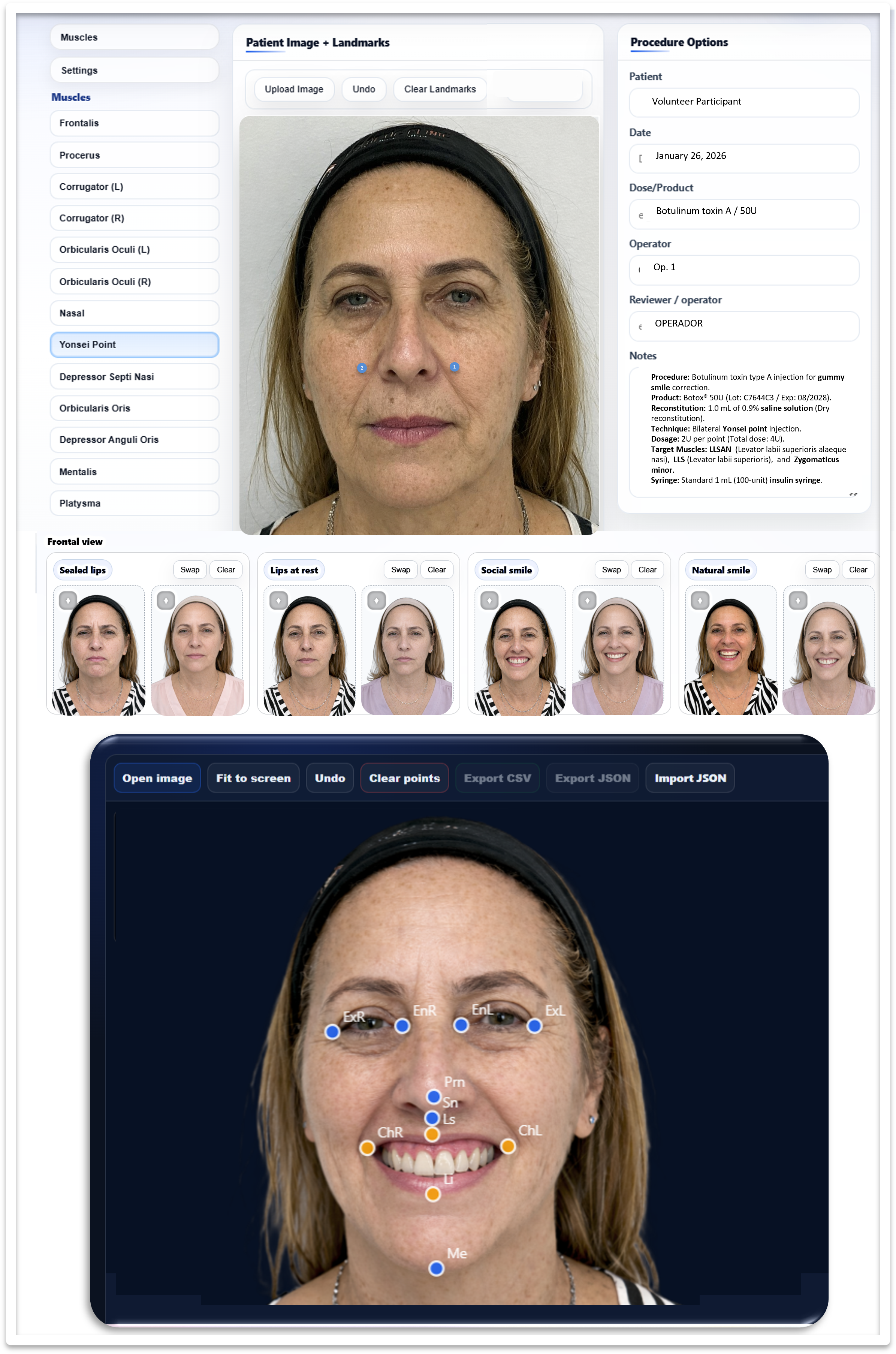
For JDHAB, the relevant shift is from informal landmark-based documentation to digitally auditable clinical targeting. Contemporary workflows can link standardized capture, structured metadata, session-based point mapping, landmark annotation, calibration fields, and exportable records within a single traceable object.
Minimum reporting checklist
| Domain | Minimum items to report | Why it matters |
|---|---|---|
| Phenotype and indication | Predominant etiology; inclusion criteria for muscular cases; excluded or co-managed factors. | Mixed etiologies distort apparent efficacy. |
| Anatomical targeting rationale | Point selected; intended muscles; symmetry logic; whether the Yonsei point was fixed, adapted, or comparative. | Named landmarks are not analytically interchangeable unless anatomical logic is explicit. |
| Product and reconstitution | Formulation, vial size, reconstitution volume, final concentration, timing, and traceability details. | Preparation conditions affect delivered product behavior. |
| Injection map and dose logic | Units per side, volume per point, depth, needle details, number of points, and retouch strategy. | Dose alone does not describe delivery architecture. |
| Capture and measurement protocol | Camera geometry, lighting, background, head orientation, smile task, calibration, software, landmarks, and endpoint definition. | Weak endpoint control can mimic or mask treatment effect. |
Knowledge gaps and practical research agenda
The key unresolved question is no longer whether BoNT/A may work in gummy smile, but why it works unevenly across patients and study designs. Future work should prioritize anatomically explicit cohort selection, full reporting of product preparation and delivery variables, and prospectively defined endpoints with documented repeatability.
For JDHAB, a practical agenda is clear: standardized frontal and profile capture; explicit smile-task instructions; internal metric calibration when justified; validated 3D surface imaging where available; session-based injection mapping; and prospective comparisons between surface-landmark targeting and digitally enhanced localization strategies.
Conclusion
BoNT/A is a defensible minimally invasive option for gummy smile when confined to compatible muscular etiologies and interpreted through a disciplined, anatomically informed protocol. Current evidence supports anatomical plausibility and short-term clinical usefulness in selected cases, but it does not justify anatomical universalization or tacit equivalence among protocols that differ in phenotyping, product handling, delivery, and endpoint capture.
The field will advance most convincingly not by multiplying named target points, but by improving the precision of what is documented before, during, and after injection. The strongest next step is a framework that links phenotype classification, anatomically explicit targeting, full reporting of preparation and delivery variables, calibrated digital capture, structured metadata, and repeatable measurement within one auditable workflow.
Required statements
Ethics approval: Not applicable.
Consent to participate: Not applicable.
Consent for publication: Not applicable. The manuscript does not report identifiable participant information.
Competing interests: Replace the blinded-review placeholder here before final scheduling for publication.
Funding: Replace the blinded-review placeholder here before final scheduling for publication.
Data availability statement: No new datasets were generated or analyzed for this review article.
Code availability statement: Not applicable.
AI use disclosure: Generative AI-assisted language editing was used during manuscript revision. The author reviewed, validated, and approved the final content and remains fully responsible for the manuscript.
Selected references
- Lacy DB, Tepp W, Cohen AC, DasGupta BR, Stevens RC. Crystal structure of botulinum neurotoxin type A and implications for toxicity. Nat Struct Biol. 1998;5(10):898-902.
- Polo M. Botulinum toxin type A (Botox) for the neuromuscular correction of excessive gingival display on smiling. Am J Orthod Dentofacial Orthop. 2008;133(2):195-203.
- Mazzuco R, Hexsel D. Gummy smile and botulinum toxin: a new approach based on the gingival exposure area. J Am Acad Dermatol. 2010;63(6):1042-1051.
- Booysen M, Becker P, Lemmer J, Lemmer P. Establishing standards for Yonsei point in a White South African population. Clin Exp Dent Res. 2023;9(5):1216-1224.
- Gong X, Tang HN, Zhang AR, Wang Z, Tang ZH, Han XF, et al. Application of botulinum toxin at the Yonsei point for the treatment of gummy smile: a randomized controlled trial. Plast Reconstr Surg. 2024;153(4):711e-721e.
- Ayaz I, Shaheen E, Aly M, Shujaat S, Gallo G, Coucke W, Politis C, Jacobs R. Accuracy and reliability of 2-dimensional photography versus 3-dimensional soft tissue imaging. Imaging Sci Dent. 2020;50(1):15-22.
- Rho NK, Bae GY, Choi MS, Chung WK, Kim HY, Kim HM, et al. Consensus on the cosmetic use of a novel botulinum neurotoxin type A product (NEWLUX®) for facial expression muscles: 2024 guidelines and discussions by Korean experts. Toxins (Basel). 2025;17(2):61.